 Annotations were performed using the following imaging inputs:
Annotations were performed using the following imaging inputs:
- Digital mammography
- Digital breast tomosynthesis (DBT)
- Synthetic mammography images (when available)
- Corresponding radiology reports, which served as the primary reference standard
- Histopathological reports (when available)
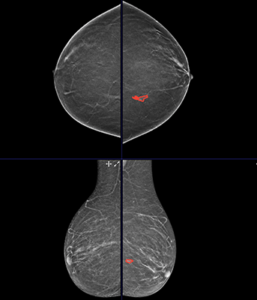
All standard mammographic and tomosynthesis views were reviewed. Lesions were annotated across all views and slices where clearly visible.
The primary objective of the protocol was to extract detailed lesion-level and study-level information from radiology reports and accurately map these findings onto corresponding imaging data through structured classification and pixel-level segmentation.
Radiologists carefully reviewed the associated radiology report before initiating image annotation. The report served as the primary source of reference and provided critical study-level and lesion-level information, including:
Study-level parameters:

- Breast density (BI-RADS A–D)
- Overall BI-RADS assessment category (0–6)
- Breast composition
- Final impression and diagnostic summary
- Histopathological reports (when available)
Lesion-level parameters:
- Number of lesions
- Laterality (left or right breast)
- Lesion type (mass, asymmetry, architectural distortion, suspicious calcification, etc.)
- Lesion size
- Lesion-specific BI-RADS category (if provided)
- Histopathological information (if available)
Radiologists used this report-based information to guide subsequent annotation and classification.